

Abstract
Community-based Birth Attendants (CBAs) provide maternally, child, sexual and reproductive information and services to a large part of the population in rural, marginalized, and hard-to-reach communities (especially in underdeveloped and developing regions). In Nigeria, they cater to ~70% of the reproductive population who patronize them in their various communities due to accessibility, affordability, and social acceptance for pregnancy-related care, delivery, and other sexual and reproductive healthcare concerns. CBAs could be skilled, and semiskilled but are largely unskilled. Their level of skill, knowledge, attitude, and practice in their community concerning different health issues is a huge determinant of their clients’ health outcomes, which has also been skewed over time. Studies have shown that the knowledge of these CBAs continues to be impeded despite attempts at training them and unifying their practices, due to the deep-seated disunity that affects their uptake of thought interventions. These divisions are drawn along the lines of religion, initial training/education, and gender differences. Therefore, continuous education on safe and current hygienic practices; increases their capacity, knowledge, and skills for correct information dissemination and service delivery. Likewise, future assimilation into the formal health system with a legal framework will help regulate their practices, thereby reducing maternal and child morbidity and mortality.
1. Introduction
Maternal health, which is a core part of women’s health during pregnancy, childbirth, and the postpartum period, contributes massively to attaining an optimal public health state, as women make up half of the world’s population and economies for development.
Pregnancy and childbirth should be joyous experiences for every woman and her household. However, this is not the case for some families as the joy is cut short at delivery, and a joyous occasion becomes a tragedy. Beyond the family, these deaths have detrimental effects on the socio-economic aspects of a country and the world at large.
Several factors contribute to these deaths, which are caused chiefly by the lack of appropriate care during pregnancy, childbirth, and post-delivery periods, with the bedrock of this care ingrained in the community. Community-based Birth Attendants (healthcare providers) provide this care for approximately 7 out of 10 women of reproductive age.
2. Maternal and child mortality: incidence, causes and implications
Maternal mortality is defined as the loss of a woman’s life resulting from pregnancy complications or death within 42 days after childbirth, notwithstanding the period or site of the pregnancy, emanating from issues that are linked to or escalated by the management of the pregnancy but from accidental or incidental causes. Whereas, Early childhood mortality includes Neonatal mortality (the probability of a child dying within the first month), Infant mortality (the probability of dying before the first birthday), Post-neonatal mortality (the difference between infant and neonatal mortality), Child mortality (the probability of dying between the first and the fifth birthday) and Under-5 mortality (the probability of dying between birth and the fifth birthday).

Every year, women’s lives are lost to complications of childbirth and pregnancy. According to the World Health Organisation, in 2017, 810 women died every day from preventable causes related to pregnancy and childbirth, with 94% of these deaths occurring in low and lower-middle-income countries. In Nigeria, maternal mortality is reported to be 545 deaths per 100,000 live births and is currently known to have the second-highest number of maternal mortality (making up approximately 20% of all global maternal mortality) and perinatal mortality in the world, with unskilled TBAs assisting up to 90% of the deliveries that lead to these high statistics.
Maternal deaths are due to complications that arise either during pregnancy or as a result of childbirth. While some conditions may exist before the pregnancy, the state of pregnancy can potentially worsen them. According to the WHO’s International Classification of Diseases-Maternal Mortality (WHO ICD-MM), maternal deaths can be direct, indirect, or unspecified.
The direct causes are those resulting from obstetric complications of the pregnancy state, be it pregnancy, labor, or puerperium), including those related to interventions, omissions of treatment, or a combination of all. These include unsafe abortions, obstructed labor, excessive blood loss, and infections. On the other hand, indirect deaths result from previously existing diseases or diseases developed in the pregnancy state that was aggravated by the physiologic effects of pregnancy. These include anemia, high blood pressure, and sugar, malaria, and heart disease.
The common most reported causes of maternal deaths in Nigeria, direct and indirect, are obstetric haemorrhage leading to anaemia, pregnancy-induced hypertension, obstructed labour, unsafe abortion, ectopic pregnancy, placenta abruptio, ruptured uterus and puerperal sepsis.
According to Odeyemi et al. also Maduka and Ogu
Other unspecified maternal deaths are those during pregnancy, childbirth, or puerperium for which the underlying cause cannot be determined. These are further divided into nine groups, which are; Pregnancies with abortive outcomes; Hypertensive disorders in pregnancy, childbirth, and the puerperium; Obstetric hemorrhage; Pregnancy-related infection such as Human immunodeficiency virus/acquired immunodeficiency syndrome, and malaria; Other obstetric Complications; Unanticipated complications of management; Non-obstetric complications; Unknown/undetermined and finally, Coincidental causes.
When women die, there are social and economic consequences that extend beyond her family. For the children left behind, evidence shows increased mortality risk, decreased nutrition, and higher chances of not going to school. There is also the consequence of a reduced labor force for the community, which results in reduced productivity. There is evidence to show that maternal mortality has a statistically significant negative effect on GDP in the WHO African region.
In most instances, maternal deaths are preventable. This is possible through timely management of mothers by skilled professionals in an environment that is supportive and adequately equipped. Skilled professionals in this context are not limited to doctors, nurses, or midwives. They include those health workers who live within the community, such as the Community-based Birth Attendants (CBAs) and other healthcare providers.
3. CBAs as a strategy to reduce maternal and child mortality
Traditional birth attendant (TBA), which makes up the large part of CBAs, according to the World Health Organisation, is a person (usually a woman) who assists a pregnant woman in childbirth; she may have acquired her skills by delivering her babies alone or by working with other TBAs. Other groups also classified and acting as CBAs are CHOs, CHEWs, JCHEWs, auxiliary nurses, faith-based birth attendants, and even some trained midwives and nursing officers who offer service at homes and in the communities away from health facilities. In contrast, a trained or skilled TBA “is an individual who has received a form of short course training to enhance his/her knowledge and skills through the modern health care sector.
Over 50% of the 130 million deliveries globally are attended to by Community-based and Traditional birth attendants. These Community-based healthcare providers are largely unskilled (i.e. TBAs) and have no formal education or knowledge on the management of childbirth-related complications, while some are semiskilled or with outdated skills (i.e. auxiliary nurses) and, therefore, are unable to prevent or treat these complications during pregnancy or childbirth that leads to maternal and/or perinatal morbidities and mortalities.
Significantly, Women of reproductive age living in developing and underdeveloped areas with weak health systems and suboptimal healthcare delivery – account for 94% of all maternal mortality globally where an estimate of about 45% of the death occurred during pregnancy; 35% during childbirth, and 20% during the postpartum period – continue to make use of TBAs during childbirth. This causes a negative ripple effect, with the unideal, inappropriate, and unethical practice steadily increasing.
Even though reports have shown a reduction in the maternal mortality rate over the years, this reduction rate has been very slow. The 2018 National Demographic Health Survey from Nigeria showed that skilled providers assisted 68% of births in urban areas compared with only 28% in rural areas, leaving the remaining 72% to the help of other unskilled Community-based Birth Attendants (CBAs) and other healthcare providers. Also, the study reflected that about 60% of the women in rural areas had a problem with accessing healthcare. These gaps highlight the importance of the availability of skilled community to women needing their services the most for necessary care.
A study done by Fagbamigbe et al. in 2017, to identify the cause of the marginal decline in maternal mortality rate in Nigeria identified increased use of skilled birth attendants during delivery. The study showed a 6% increment in the use of skilled birth attendants between 1990 and 2013. The World Health Organisation also recorded a drop in maternal mortality rate by 53% during that period. Some of the factors responsible for the increased rate of skilled birth attendants use include creating the national midwives’ service scheme, equipping primary health care centers, providing empowerment programs, and so on. Other determinants affecting women’s usage of skilled birth attendants include proximity to the health facility, socio-economic status, and previous positive experience.
Regarding health equity, the role of community birth attendants also comes to mind as they help ensure that women in rural communities are not left behind in terms of their maternal health care. Aside from being instrumental and playing a massive role in reducing maternal mortality, they also provide certain personalized care for their patients such as; counseling, home visitations, support during labor, charging cheaper rates, and allowing for payment of services by barter or in installments. This is quite important for most women as a report has shown that the perception of skilled birth attendants as being hostile and disclosing confidential information are some of the hindering factors to receiving care from skilled birth attendants. Therefore, to significantly reduce the burden of maternal mortality in Nigeria, the role of the CBAs is of crucial importance and cannot be undermined.
4. Integration of CBAs in health service provision
The UN sustainable development goal to reduce the global maternal mortality ratio to <70 per 100,000 live births by 2030 seems impossible due to the prevalence of high maternal mortality rate globally (211 deaths per 100,000 live births in 2017) and in developing countries, especially Nigeria where there were about 917 deaths per 100,000 births in 2017. This is a product of these places’ weak operational health systems – lacking well-trained, adequately informed, technology and quality inclined healthcare providers, well-maintained and equipped facilities, logistics, and functional policies. Likewise, studies have shown that the risk of maternal and perinatal death is increased dramatically when there is unskilled birth assistance (done mainly by TBAs and other CBAs).
The health workforce is the bedrock to achieving a good health system and its outcome. Hence, every healthcare provider, including the CBAs – who is a link between the community and health service providers especially, skilled birth attendants, and are always available, accessible, affordable, and socioculturally acceptable in communities (especially the low socio-economic, rural, underserved, hard-to-reach and grassroots) – cannot be ruled out of the optimal healthcare provision and human resources allocation.
Due to this, including the slow uptake and shortage of SBAs, several countries have opened up the proposal to officially adopt CBAs as part of the flowchart for maternity care and attempted to integrate CBAs into their health system – following the failure to suppress them. However, the results and techniques have differed from LMIC like Bangladesh and Kenya to HIC like China. Nevertheless, studies have shown that health education and training programs for TBAs are instrumental in upskilling them to promptly recognize warning signs of emergencies and know when to transfer the woman to the hospital.
Integrating them into the health system in Nigeria is challenging because, despite the widespread acceptance and use of these service providers, they are illegal. This is one of the major bottlenecks in integrating them into health services. Due to this problem, they can only function within the limits of the law as referral points, and points of community entry, and they can help prevent harm to the mother and child. However, there is not enough SBA in the country, and as a result, policies such as task shifting and sharing will need to be adjusted to reflect and accommodate the current circumstance.
The first step has to eliminate this problem and recognize them legally with well-defined roles and limits to serve their communities. They can regularly report to the local government medical officers, primary health centers, or the public health board with frequent assessments and updated recertification training. Some of the Knowledge and skills for procedures needed to ensure safe delivery and maternal and perinatal survival are the proper use, and implementation of aseptic techniques, uterotonics, anticonvulsants, antibiotics, blood transfusion, and more is lacking among them. Therefore, they should be trained to prevent and recognize complications by teaching them significant aspects of maternal care, including Family planning (FP), Misoprostol Use, Measurement of blood loss, Antepartum care, normal labor, Postpartum care for mothers, Postnatal care for neonates and so on. However, very importantly, this knowledge and skills should be fashioned and effectively implemented to fit their cadre, strict community level duties, in line with the task shifting and sharing policy in Nigeria.
5. Presumptive actions of CBAs in maternal healthcare service delivery
In the majority of the countries most affected by maternal mortality, uptake of family planning is low. Given that the CBAs are usually respected voices or authorities in their community, training them on family planning counseling and making them advocates will make it more appealing to the women. There is also a personal relationship and closeness between CBAs and their patrons still largely absent in the typical hospital or clinic dynamic. A reduction in the number of birthing events correlated strongly with a decrease in maternal deaths.
Years ago, the prevention or treatment of postpartum hemorrhage in small villages or towns without electricity or the need for injections was near impossible. For example, in LMICs like Tanzania, they estimate blood loss using the quantity of soaked clothes fabrics and can be taught other standardized methods that are excellent steps at spotting postpartum hemorrhage. They can learn the local equivalence of 500mls of blood to know when to refer the women for advanced and emergency care in health facilities. Also, with the advent of misoprostol, it is possible to train these CBAs to administer it safely in their centers. This will reduce the risk of death due to postpartum hemorrhage, reducing one of the most emergent causes of maternal mortality.
CBAs can also encourage their patrons to get advanced care after birth and take vaccines in health centers. These are aspects of care that the majority of the CBAs generally do not offer in their regular plans, especially postpartum care. Notably, attempts to use the “promise of financial compensation” to encourage the CBAs to refer their clients to the hospital for postpartum care have shown varying results. Teaching CBAs to clean women and care for them and their babies after delivery can save many lives lost to maternal and child mortality.
Likewise, CBAs having good knowledge and counseling skills on HIV/AIDS and Prevention of Mother-To-Child Transmission of HIV (PMTCT) with good knowledge of specific measures of infection prevention and control can help them to protect themselves, their patients, and the entire community while opting for orthodox medicine as the management of the various viral infection (COVID-19 inclusive), rather than the use of native or herbal remedies to cure them.
All of these and more training, regular feedback, and a proper referral system will help create a genuinely integrated health service that has the interests of the healthcare consumers at the fore of its priorities. Hence, this is not the time to “gatekeep” but to be proactive by integrating CBAs via a full-on multifaceted project because human resources for health, including SBAs, are not growing fast enough to meet the community’s needs. Therefore, all the stakeholders should be given a seat at the table to deliberate the methods, limits, appropriate policies, and legislation.
6. Challenges and progress so far: discussion of field reports
Various challenges exist that hinder the maximization of CBA roles to reduce maternal and child mortality and the general healthcare provision system as a whole. These challenges have been identified through an extensive review of literature and fieldwork.
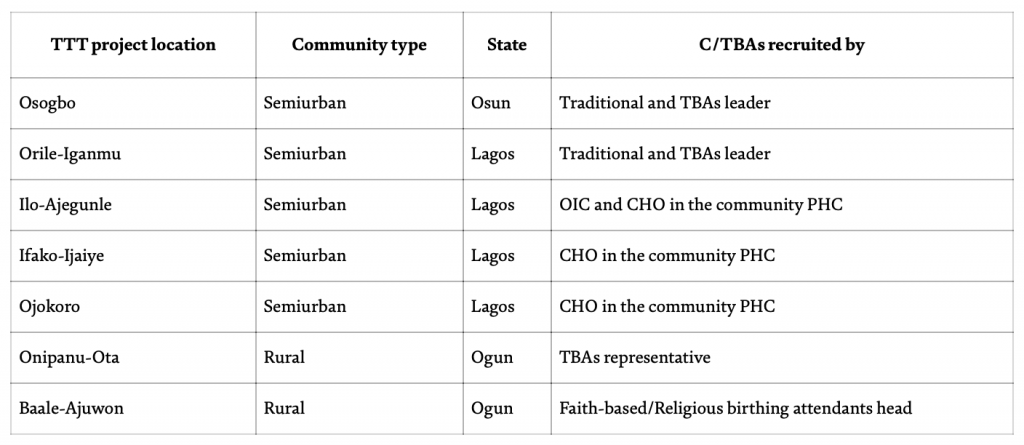
Through our field works of Training-The-T/CBAs (Project TTT) at SHI, 162 CBAs have been reached since 2018, and some of the issues common to them irrespective of location are palpable ignorance and reluctance to learn or adopt new methods. This reluctance is influenced by their confidence in their old traditional ways and how long they have been using them and getting away with the outcomes. For example, during the FGD on family planning before TTT at Orile-Iganmu (a Semi-Urban community in Lagos state, the megacity of Nigeria), the head of the TBAs (a herbalist) that has practiced for over 30 years and trained countless other TBAs stated confidently in his native language and translated that “BTL is tying of the cervix and meant for people that have done abortions in the past because their cervix and vagina have become wide and the “spring“ there does not close. Therefore, the other forms of contraceptives like OCPs and condoms do not work for them…”; whilst only 2 of the 162 CBAs reported that FP prevents (unsafe) abortion and none of them reported that FP prevents STIs in their pre-assessment questionnaires.
Also, other aspects found to be erroneously managed and discussed among them during an FGD among the same cohort and another recruited into the TTT Project in Ilo-Ajegunle (another semi-urban community in Lagos) were postpartum psychosis during and after labor, partners’ inclusion in family planning, postdated pregnancy lasting up to one and half years, exclusive breastfeeding and other breastfeeding issues. Likewise, immunization of mother and child and efficient data collection of their activities with the client was also lacking among the majority.
NB: n is the total number of Birthing Attendants reached by the TTT Project.
Data collection was by self-administered semi-structured questionnaire, interview-based and Focused Group Discussions. Data collation was between January 2018 till March 2021.
NB: n is the total number of Birthing Attendants reached by the TTT Project.
Another occurrence was during the FGM session at the same training in Osogbo (the capital of the traditional and religious state), where more than 80% of the participant CBAs vehemently supported that FGM was compulsory family tradition and the right to protect the female. Also that they relied on their “Opele” – divining oracle – and herbs for complex and prolonged/obstructed deliveries rather than refer to a health facility, which has been working for them. However, the untold consequences of these actions and strong beliefs are the morbidity and mortality cases recorded among the mothers and babies that patronize them when they return home to commence their everyday lives. Some of the highlighted morbidity outcomes in the babies leading to permanent damage are neonatal jaundice, and mismanagement of the first golden minute of life. While in the mothers are puerperal sepsis, and postpartum hemorrhage, to mention a few.
Furthermore, another challenge was the lack of a comprehensive and all-inclusive database of every functioning CBAs in communities despite having a regulating body or a converging association or point of meeting with their assigned CHOs in their resident community PHCs. Hence, they cannot all be tracked, trained, or their activities monitored, with some even hiding under the guise of running a “private hospital” instead of the actual traditional homes or centers they run. These can be due to age, level of exposure, type and level of education/training, the difference in religion, location/locality, beliefs, and practices.
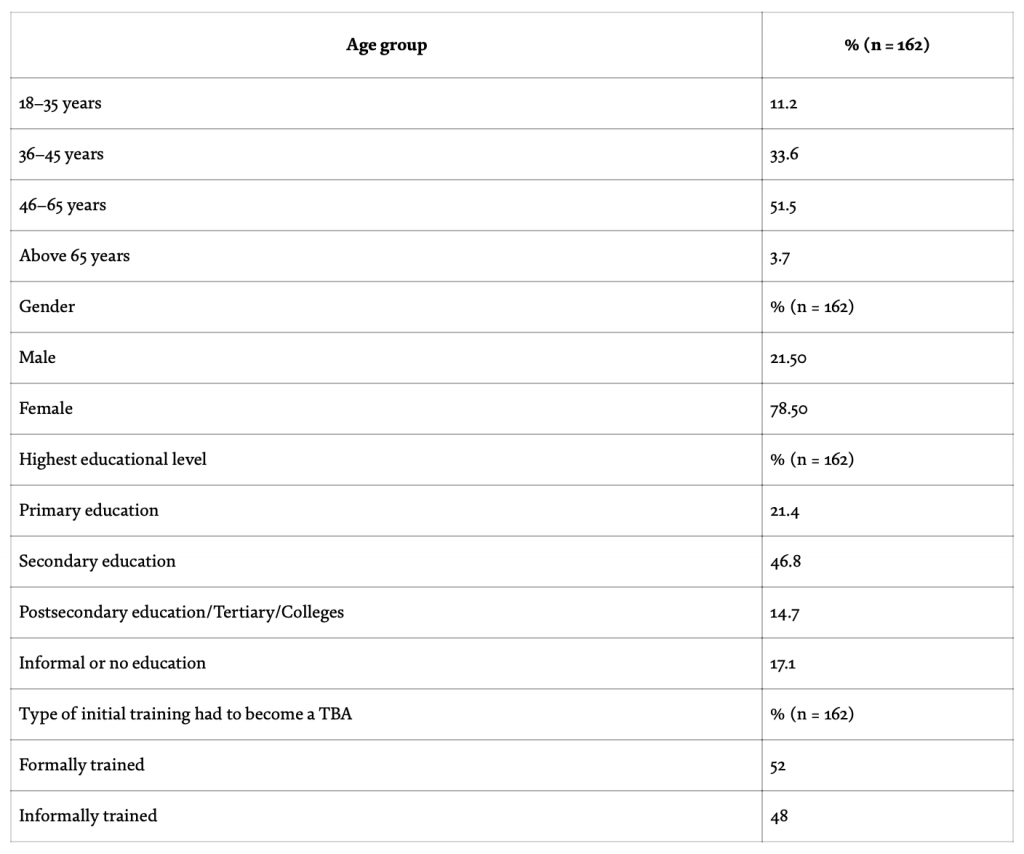
Some evidence supporting this from data collated through our TTT project showed that of the 162 reached and trained; 51.5% were between the ages of 46–65, 33.6% between 36 and 45 years, rarely the elderly who trained them showed (they made up only 3.7%) and the young one who is currently receiving the informal training (18–35 years’ participant made up just 11.2%). Keep in mind that age should not be a limitation to acquiring knowledge. Likewise, primarily those who had some form of formal training wanted more, as 52.0% of participants had some formal training to become birth attendants or community healthcare providers versus 48.0% who were informally trained. While 21.4% had primary education, 46.8% had secondary education, 14.7% had postsecondary education (including college of health technology), and 17.1% had informal or no education.
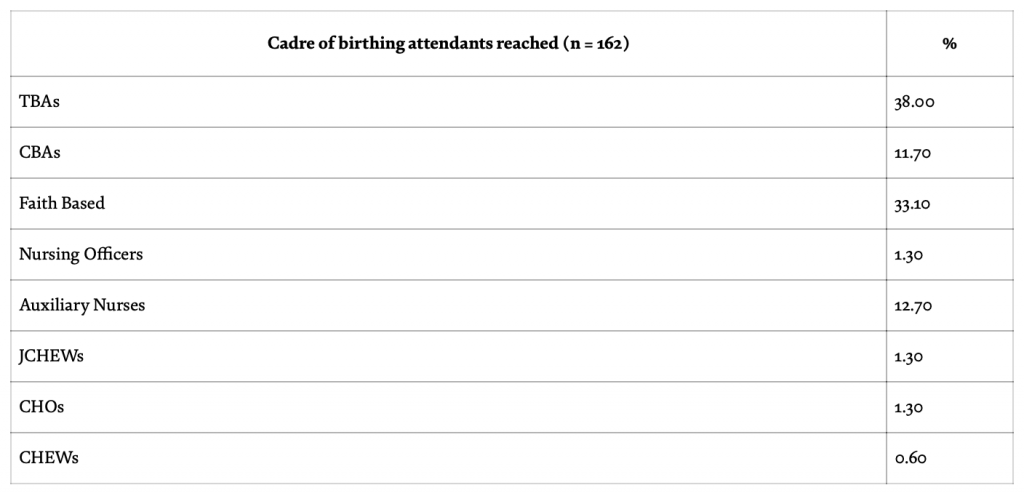
Furthermore, the percentage of all participants attending the training by qualification and initial training was recorded; 38.0% were TBAs, 33.1% were faith-based birth attendants, 12.7% Auxiliary nurses, 11.7% CBAs, 1.3% Nursing Officers, 1.3% CHOs, 1.3% JCHEWs and 0.6% CHEW (SHI 2020 Annual report) [24]. This lower attendance of CBAs with higher qualifications might be attributed to the perceived need or aim for more training, mode of community entry, reachable circle, and target of CBAs mobilizer.
At a community entry meeting with one of the CBAs by the SHI strategy team (i.e. the contact person we were able to reach) in Baale-Ajuwon (a rural community in Ogun state), she emphasized in her native language that “as a faith-based CBA, I try not to mingle with the TBAs because of their diabolic ways…”, hence for the training would only reach out to the faith-based CBA like herself. This also shows the disharmony between the cadres of CBAs hindering them from learning and benefiting from each other to progress and be able to offer the best to their clients. Also, the participant sex percentage was 21.5% male to 78.5% female. It was found that where women were the CBA leaders, mostly women only tend to come for the training and be more expressive, as opposed to where men were the leaders – the meetings were more dominated by men with women less expressive and taking permission from the men to air their opinions. This shows the gender disparity and inequality even at the level of community health care.
However, despite these challenges hindering their roles, some progress has been made such as the increase in the knowledge and attitude towards FP, Safe delivery, hygiene practices in the workspace, immunization, exclusive breastfeeding and empowerment with IEC and educative materials for themselves and their clients; all of which play a huge role in reducing maternal and child morbidity and mortality in their communities and the world at large. During follow-up visits to the CBAs in FDG, they report more patronage on account of the free birthing kits and FP counseling services they offer – courtesy of the Safer Hands Health Initiative.
7. The future and CBAS: recommendations
Currently and in the nearest future, the “irreplaceable” roles of CBAs in healthcare delivery services cannot be dismissed or disregarded. Hence, prompt actions must be taken to reduce the maternal, perinatal, and child morbidity and mortality in Nigeria and globally associated with them. Some of which include;
Legalizing the roles of CBAs and building a controlled framework to integrate them into the formal healthcare system. Also, incorporating community stakeholders’ input and participation can help improve healthcare service delivery and programs.
Strengthening effective communication between CBAs and skilled health workers to avoid disharmony and counter-productivity in the grassroots healthcare system. This can be achieved by creating a conducive and functional referral system and emergency line for CBAs to their community healthcare centers or medical practitioners in charge. This would also increase their access to healthcare facilities.
Training, educational conferences, and empowerment at all levels (local, national, and international) should be periodically and continuously done to cross-learn from what is obtainable and yield positive outcomes in other developed places. Also, with a day dedicated to them (i.e. International day of CBAs) to recognize their ethical works, referrals, and reported/documented activities. This would inform their activities, and exposure and incline them towards quality care delivery.
Likewise, incentivizing their efforts to recruit a robust database of every CBAs in their communities – as they know themselves – and enroll their trainees for proper/formal healthcare training in schools. Incentives could be per referral/enrollment or after a target number set is met, and it could be in the form of money, materials, or more opportunities like scholarships for formal enrollment, training, and attachment in recognized institutions. This would encourage them to come out, be trained, and get acquainted with policies, protocols, infrastructural, and healthcare advancements. Owing to the fact that over 50% of the TTT participants reported that government policies had no impact on their activities and approximately 40% had no idea of any government policies affecting their work, while only about 9% reported that the government was putting in some efforts to make their works good but can still do better.
Finally, increasing quality community health education for women, men, and their families – which is socioculturally appropriate and sensitive – is essential. As this would inform their healthcare decisions, improve their health-seeking behaviors, and positively influence paternal attitudes towards healthcare which is also an important factor for the overall well-being and economic status of women and their families.
8. Conclusion
Birth attended by CBAs, especially TBAs, is associated more with maternal and child morbidity and mortality in Nigeria and globally, as most TBAs are unskilled. Currently, Nigeria is leading in maternal and child morbidity and mortality with the high patronage of TBAs as opposed to a skilled birth attendant or going to health facilities. Therefore, to reduce these maternal and perinatal deaths and, in turn, achieve the global Sustainable Development Goals (SDGs), it is pertinent to upscale the role of these CBAs for more skilled birth attendance and other delivery services by training them and possibly integrating them into the formal health system.
WRITTEN BY: Mary Agoyi, Roland Ojo, Toyosi Afolabi, Olakunmi Ogunyemi, Sekinat Adejumobi and Adeyemi Awoniyi
Acknowledgments
The author(s) would like to acknowledge the entire members of the CBA groups reached out to across various communities for making this possible, the CHOs and IOC who served as mobilizers, Prof. Kofo Odeyemi for her continuous supervision of the project, Dr. Doyin Ogunyemi for her contributions and Birthing Kit Foundation Australia (BFKA) for their continuous provision of birthing kits used as incentives for the CBAs.